


 Sign Out
Sign Out

The frequencies reported in the table as follows are derived from clinical trials in the metastatic and adjuvant settings (having included 416 and 1108 patients respectively in the oxaliplatin + 5-FU/FA treatment arms) and from post marketing experience.
Frequencies in this table are defined using the following convention: very common (> 1/10), common (> 1/100, ≤ 1/10), uncommon (> 1/1000, ≤ 1/100), rare (> 1/10000, ≤ 1/1000), very rare (≤ 1/10000) including isolated report.
Further details are given after the table. (See Table 7.)
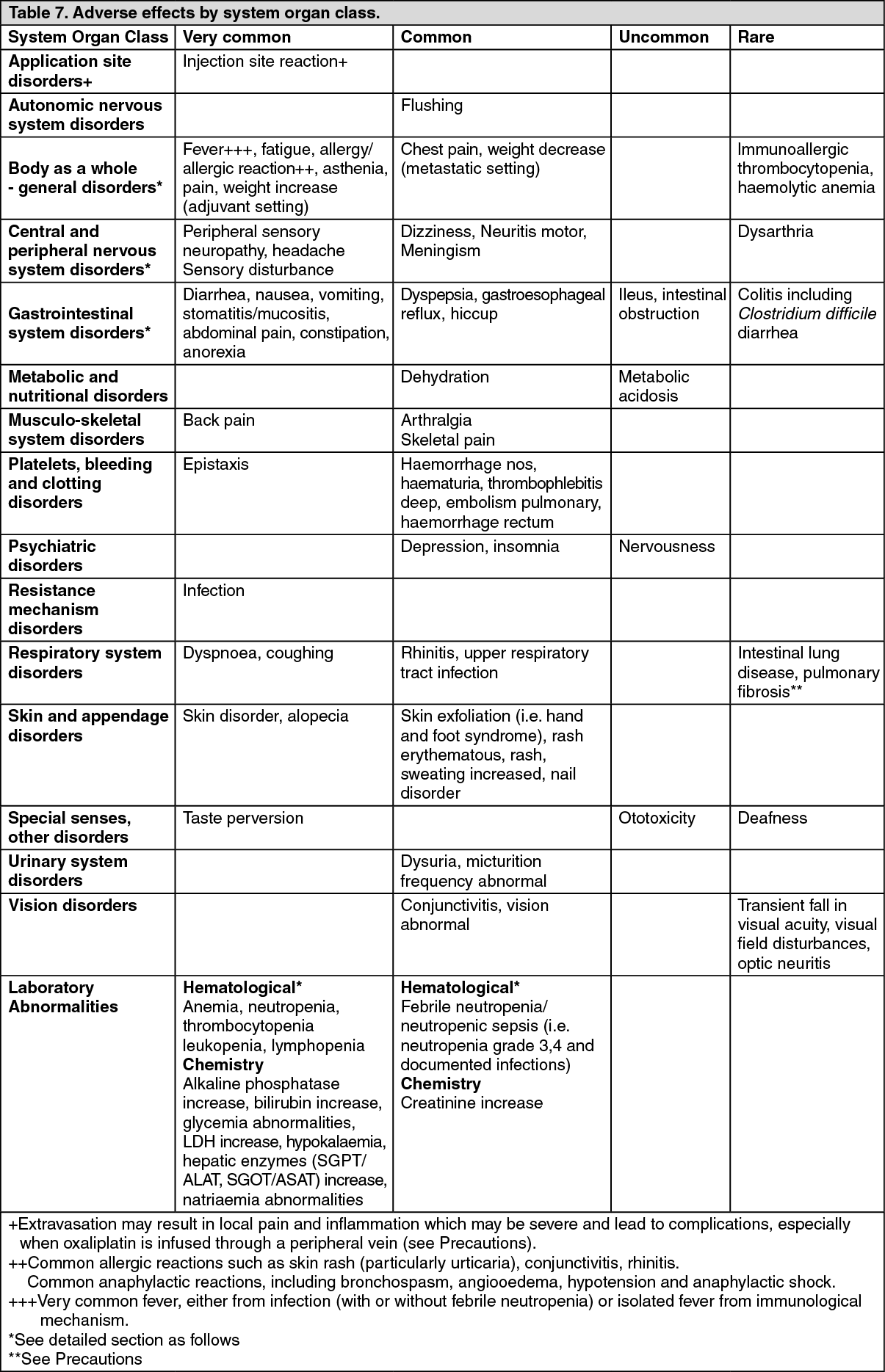 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHaematological toxicity: See Table 8.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDigestive toxicity: See Table 9.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageProphylaxis and/or treatment with potent antiemetic agents is indicated.
Dehydration, paralytic ileus, intestinal obstruction, hypokalemia, metabolic acidosis and renal impairment may be caused by severe diarrhoea/emesis particularly when combining oxaliplatin with 5-fluorouracil (see Precautions). In single cases pancreatitis is reported.
Nervous system: The dose limiting toxicity of oxaliplatin is neurological. It involves a sensory peripheral neuropathy characterized by dysaesthesia and/or paraesthesia of the extremities with or without cramps, often triggered by the cold. These symptoms occur in up to 95% of patients treated. The duration of these symptoms, which usually regress between courses of treatment, increases with the number of treatment cycles.
The onset of pain and/or a functional disorder are indications, depending on the duration of the symptoms, for dose adjustment, or even treatment discontinuation (see Precautions).
This functional disorder includes difficulties in executing delicate movements and is a possible consequence of sensory impairment. The risk of occurrence of persistent symptoms for a cumulative dose of 850mg/m2 (10 cycles) is approximately 10% and 20% for a cumulative dose of 1020mg/m2 (12 cycles).
In the majority of the cases, the neurological signs and symptoms improve or totally recover when treatment is discontinued. In the adjuvant setting of colon cancer, 6 months after treatment cessation, 87% of patients had no or mild symptoms. After up to 3 years of follow up, about 3% of patients presented either with persisting localised paraesthesias of moderate intensity (2.3%) or with paraesthesias that may interfere with functional activities (0.5%).
Acute neurosensory manifestations (see Pharmacology: Toxicology: Preclinical safety data under Actions) have been reported. They start within hours of administration and often occur on exposure to cold. They may present as transient paraesthesia, dysaesthesia and hypoesthesia or as an acute syndrome of pharyngolaryngeal dysaesthesia. This acute syndrome of pharyngolaryngeal dysaesthesia, with an incidence estimated between 1% and 2%, is characterised by subjective sensations of dysphagia or dyspnoea, without any objective evidence of respiratory distress (no cyanosis or hypoxia) or of laryngospasm or bronchospasm (no stridor or wheezing); jaw spasm, abnormal tongue sensation, dysarthria and a feeling of chest pressure have also been observed. Although antihistamines and bronchodilators have been administered in such cases, the symptoms are rapidly reversible even in the absence of treatment. Prolongation of the infusion helps to reduce the incidence of this syndrome (see Precautions).
Other neurological symptoms such as dysarthria, loss of deep tendon reflex and Lhermitte's sign were reported during treatment with oxaliplatin. Isolated cases of optic neuritis have been reported.
Allergic reactions: See Table 10.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form